[This article is excerpted from a talk given June 17, 2021, at the Mises Institute’s Medical Freedom Summit in Salem, New Hampshire.] Ladies and gentlemen, why are we here today? First, in a certain sense medicine in America is broken. Doctors and patients are unhappy, the quality of care deteriorates, and costs keep increasing. Even before covid, US life expectancy declined three years running. Even before covid, too many Americans were sick, depressed, fat, and unhappy with their physical and mental health. I wonder if we’ll ever have accurate data about undiagnosed and untreated cancer and other serious illness as a result of the hospital and clinic lockdown. It strikes me this is the kind of information we might want before we consider another lockdown for any
Topics:
Jeff Deist considers the following as important: 6b) Mises.org, Featured, newsletter
This could be interesting, too:
Nachrichten Ticker - www.finanzen.ch writes Die Performance der Kryptowährungen in KW 9: Das hat sich bei Bitcoin, Ether & Co. getan
Nachrichten Ticker - www.finanzen.ch writes Wer verbirgt sich hinter der Ethereum-Technologie?
Martin Hartmann writes Eine Analyse nach den Lehren von Milton Friedman
Marc Chandler writes March 2025 Monthly
[This article is excerpted from a talk given June 17, 2021, at the Mises Institute’s Medical Freedom Summit in Salem, New Hampshire.]
Ladies and gentlemen, why are we here today?
First, in a certain sense medicine in America is broken. Doctors and patients are unhappy, the quality of care deteriorates, and costs keep increasing. Even before covid, US life expectancy declined three years running. Even before covid, too many Americans were sick, depressed, fat, and unhappy with their physical and mental health. I wonder if we’ll ever have accurate data about undiagnosed and untreated cancer and other serious illness as a result of the hospital and clinic lockdown. It strikes me this is the kind of information we might want before we consider another lockdown for any reason.
But at the very same time, medicine (broadly speaking) is absolutely poised for incredible entrepreneurial breakthroughs which will revolutionize not only the practice and delivery of medicine, but how we think about health altogether. From cash practices to medi-share programs to medical tourism and drug importation, the future promises huge innovations of the kind our speakers today will discuss—but only if we have the good sense to allow it.
One thing we cannot ignore: doctors are deeply dissatisfied. According to the 2018 Great American Physician Survey, only half of doctors would recommend the profession to young people, and less than half were happy with the direction of the profession. Their biggest complaint? Third-party interference, whether insurance or government, and correspondingly a lack of independence. Doctors think they are working harder for less money and less respect.
I’m sure most of us in this room would like to live into our eighties and nineties—and enjoy them in reasonably good health. But our golden years will be full of doctor visits, as anyone with aging parents can attest. Who will be the doctors treating us in those coming decades? Will they be the best and brightest young people? Will they forego tech or Wall Street or some more lucrative profession to spend fourteen hours per day looking at our aged feet or clouding eyes? Who will do this for $150,000 per year, as an HMO employee with little autonomy or status? Who will give up their twenties to medical school when “doctor” loses what’s left of its prestige?
So medicine desperately needs change. But what kind of changes, and decided by whom?
Fiat Medicine versus Market Medicine
It depends on which of two competing visions we accept.
The first vision is political; we’ll call it fiat medicine. “Fiat” means commanded by government, through legislative decree. We pass laws and people get healthcare, just as we pass laws and people get welfare, housing, education, entitlements, or any kind of government service.
But in this vision healthcare is truly unique, unlike any other goods or services. It can and must be provided by the state, though perhaps with some grudging overlay of nominally private but equally centralized insurance companies and HMOs, nominally private practitioners, and nominally private medical schools—as we see in France, for example, compared to the purely state model of the NHS [National Health Service] in Britain.
This vision essentially says economics is not real and incentives don’t matter when it comes to medicine. Hand in hand with this, it also decrees free healthcare as a positive right. This means how healthcare is provided, by whom, where and when, in what amounts, and in some cases even whether it is provided at all becomes a political question decided politically. In sum, this is the single-payer vision: not yet reality in America, but with growing support. How many times have you heard “The US is the only advanced country without free healthcare for all”?
The second vision we’ll call market medicine. This vision relies on investment of private capital, profit and loss, market discipline, and market signals for the allocation of resources. It accepts economics as real, which means incentives matter and the realities of supply and demand cannot be legislated away. Healthcare is not a right, but something the marketplace can deliver, and deliver better than the centralized state. And just as with private markets for all kinds of things, it recognizes a robust role for private charity in helping to care for the poorest and most infirm among us.
A third vision of sorts, one we might call crony medicine, is the current reality in America. This combines state mandate but ostensibly private insurance systems, a vast overlay of senior Medicare services paid for by taxes but provided by private doctors, and restrictive licensing of providers, drugs, and devices, which has proven hugely susceptible to regulatory capture. An observer might call this corporatism, a cynic might call it fascist.
The point is this: each of these three visions has its own touchstones, its own key aspects. Under a system of political medicine, the touchstones are public money and public bureaucracy. Under a crony system, the touchstones are lobbying influence and private bureaucracy.
Under a market system, those touchstones are scarcity and choice.
So America has to choose, either expressly or by default, which of these three visions will prevail. But if we were building an aviation system we would probably want to understand gravity and lift. Scarcity and choice are simple reality, and reality asserts itself.
The Future of Market Medicine
So what might medicine look like in a free market, or at least a freed market? One where almost all doctors, nurses, and other providers were indeed truly private market actors? One where health insurance was not mandated, where any kind of à la carte plans were allowed—from barest of bare bones to Cadillac plans—where actuarial risk and personal habits operated to set premiums, and most importantly where most care was paid for with cash rather than insurance?
We can’t know, of course—but I suspect it will look something like this (not would, will—we should be optimistic!):
- Cash for basic services and low-cost, high-deductible catastrophic insurance for serious illness or accidents;
- A healthy market in secondary insurance to cover those high deductibles;
- Cheaper and more ubiquitous long-term care policies for end-of-life costs;
- A bevy of convenient frontline options for all of those common situations, from kids with a fever to twisted ankles: think urgent care, but with the convenience, efficiency, and low prices of a competitive cash market.
- These frontline cash centers will be widely found in big-box stores, pharmacies, strip malls, and rural towns, not close to ERs;
- Cash clinics will also provide dental and eye care, along with expanded capacity for one-stop blood testing, radiology and MRI, allergy testing, mental health services, cosmetic treatments, and the like. ER visits correspondingly will fall;
- They will offer very fast or immediate appointments, with an app to let you stay comfortably at home until your visit rather than some dismal waiting room;
- Telemedicine will explode, allowing for a far greater range of maladies to be treated without seeing a doctor in person—accelerated by covid;
- Physician’s assistants and nurse practitioners will play a larger and larger role in patient care;
- Both medically necessary and elective surgery will see a revolution in pricing, with transparency and unbundling along the lines of the Oklahoma Surgery Center;
- Furthermore, the market increasingly will produce provide a range of surgery “experiences,” from bare-bones clinics to luxury experiences in resort-like settings;
- Rehabilitation and sports medicine clinics will boom—recovery and mobility become understood as part of core health;
- Demand for supplements and alternative treatments will increase as the over-65 population doubles in the coming decades, creating political pressure against greater regulation of such supplements and treatments;
- As the private market expands, price elasticity of demand will reassert itself! The kind of conscious decision-making we see today with respect to cosmetic surgery and LASIK eye surgery will cut across all forms of treatment;
- Finally, diet, stress management, personal knowledge, and personal habits will play a much bigger role in the future of medicine. Our approach to health as individuals will become more holistic. Price transparency and financial incentives will give us more ownership and accountability for our own health. If anything, the covid experience demonstrated that no one is coming to save us. Life expectancy and quality of life are in our hands; doctors and other providers are our agents, here to help facilitate things. The days of quietly and passively sitting in the examination room while doctors send us off with a pill are over.
Conclusion
None of this is fantasy. Much of this is already happening. Of course, this is not to say government will not be involved, medical licensing or FDA (Food and Drug Administration) constraints will disappear, or pure free market mechanisms will create nirvana. If anything, insolvent governments, both federal and state, will be forced to adopt or allow some degree of market discipline to deal with entitlements and healthcare costs. Social Security, Medicare, Medicaid are not going to magically go on forever. The FDA will feel pressure from a world of globally importable drugs and medical devices obtainable in other countries. Even if an outright single-payer system is adopted, the bifurcation between private and state medicine will simply accelerate. The beautiful deflationary pressure of markets will not be denied in a country of 330 million people, so kinds of care once available only to the very rich—think Barbara Streisand and her concierge doctors—will become cheaper and cheaper. And all the while, cash prices will continue to fall while insurance premia, copays, and deductibles will continue to rise—even if that insurance takes the form of Medicare for All or some state program.
So that’s really why we are here today, to talk about the space, the opportunity, provided by the diminishing delta between cash and insurance costs, between the state and the market, between the reality of scarcity and the wishful thinking of bureaucrats promoting “free” healthcare. Each of our great speakers has something insightful to say about that space.
Thank you.
You Might Also Like
 Weekly SNB Sight Deposits and Speculative Positions: Inflation is there, CHF must Rise
Weekly SNB Sight Deposits and Speculative Positions: Inflation is there, CHF must Rise
2021-06-21
Update June 21 2021: SNB intervening. Sight Deposits have risen by +1.1 bn CHF, this means that the SNB is intervening and buying Euros and Dollars.
 The Drive for State and Federal Protective Tariffs in Early America
The Drive for State and Federal Protective Tariffs in Early America
2021-02-23
Every depression generates a clamor among many groups for special privileges at the expense of the rest of society—and the American depression that struck in 1784–1785 was no exception. If excess imports were the culprit, then voluntary economizing could help matters, and the press was filled with silly fulminations against ladies wearing imported finery.
 AOC and Schumer Want Taxpayer Funding for Covid-19 Funerals
AOC and Schumer Want Taxpayer Funding for Covid-19 Funerals
2021-02-10
US residents whose family members died with or of covid will be eligible to receive $7,000 for funeral and related expenses, New York senator Chuck Schumer (D) and Representative Alexandria Ocasio-Cortez (D) announced.
 A Penchant for Controlling Others
A Penchant for Controlling Others
2021-02-06
We all want freedom for ourselves, but many people have doubts about the way others might use their own freedom. Under these conditions, the state is there to help. Get enough people to favor enough restriction, and the state is good to go, administering every aspect of life from its smallest to its largest detail.
 Biden Nominee Rachel Levine Was a Disaster in Pennsylvania. Now She’s Headed to Washington.
Biden Nominee Rachel Levine Was a Disaster in Pennsylvania. Now She’s Headed to Washington.
2021-01-25
On January 19 it was announced that Joe Biden planned to nominate Rachel Levine, the Pennsylvania (PA) secretary of health, for the position of assistant secretary of health in the Department of Health and Human Services. This is potentially good news for Pennsylvanians, who will finally be rid of her after having had to endure her disastrous covid lockdowns and restrictions for nearly a year, but is likely bad news for the rest of the country.
 The Myths Behind the “Capitalism Is Racist” Claim
The Myths Behind the “Capitalism Is Racist” Claim
2021-01-22
Though numerous studies prove the contrary, it is still widely assumed that capitalism perpetuates racism. Celebrities and academics incessantly broadcast the message that capitalism engenders racism.
 The Upside of Lockdowns: More Saving
The Upside of Lockdowns: More Saving
2021-01-18
Rothbard: “At the outset of every step forward on the road to a more plentiful existence is saving….Without saving and capital accumulation there could not be any striving toward nonmaterial ends.”
 Fiscal Stimulus vs. Economic Growth
Fiscal Stimulus vs. Economic Growth
2021-01-12
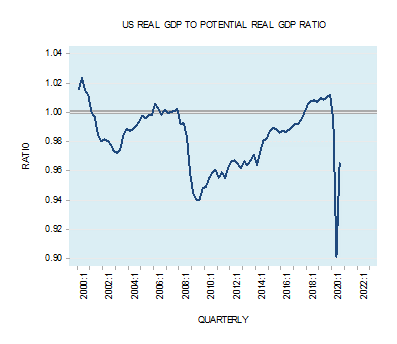
[unable to retrieve full-text content]For most experts a key factor that policymakers should be watching is the ratio between actual real output and potential real output. The potential output is the maximum output that the economy could attain if all resources are used efficiently. In Q3 2020, the US real GDP–to–potential US real GDP ratio stood at 0.965 against 1.01 in Q3 2019.
Tags: Featured,newsletter